Medical schools are changing. Textbooks and whiteboards now share space with interactive software, and students who grew up with touchscreens and gaming expect their educational tools to keep up. Game-based learning (GBL) has emerged as one way schools are responding, bringing structured, interactive play into the curriculum.
What is Game-Based Learning?
Game-based learning uses the mechanics of games (challenges, rewards, storytelling, progression systems) to teach. The core idea is straightforward: hold a student’s attention and they’ll retain more. GBL requires active participation, problem-solving, and decision-making, which is a big part of why it works.
It’s come a long way. What started as simple educational games for young learners now spans mobile apps, online platforms, simulations, and even board games adapted for professional training. The format varies, but the goal doesn’t: make learning active rather than passive.
Game-Based Learning in Medical Education
Traditional lectures work to a point, but they often don’t engage students deeply enough in subjects like anatomy and pharmacology. GBL can complement those methods in several ways:
- It holds attention more effectively than lectures by tapping into the brain’s reward system. Medical students using GBL consistently report higher engagement and enjoyment than with traditional methods alone.
- Active participation improves retention. Applying knowledge in real-time scenarios builds deeper understanding than reading or listening alone. A meta-analysis by Sailer and Homner (2020) found that GBL environments produced better learning outcomes than conventional instruction.
- Simulated clinical scenarios let students practice decision-making in a low-stakes environment, building confidence before they encounter real patients.
- GBL platforms generate performance data, giving educators a way to track progress and identify where students are struggling.
- The social layer matters too. Leaderboards, team challenges, and shared progress create accountability that solo study can’t replicate.
Garris et al. (2002) found that game-based frameworks substantially boost student motivation, which matters because motivation is what sustains the long study hours medical training requires.
Why It Works for Neuroanatomy
Neuroanatomy is notoriously difficult. The structures are complex, the spatial relationships are hard to picture from flat diagrams, and neural pathways can feel abstract in ways that textbooks struggle to convey. GBL addresses several of these problems:
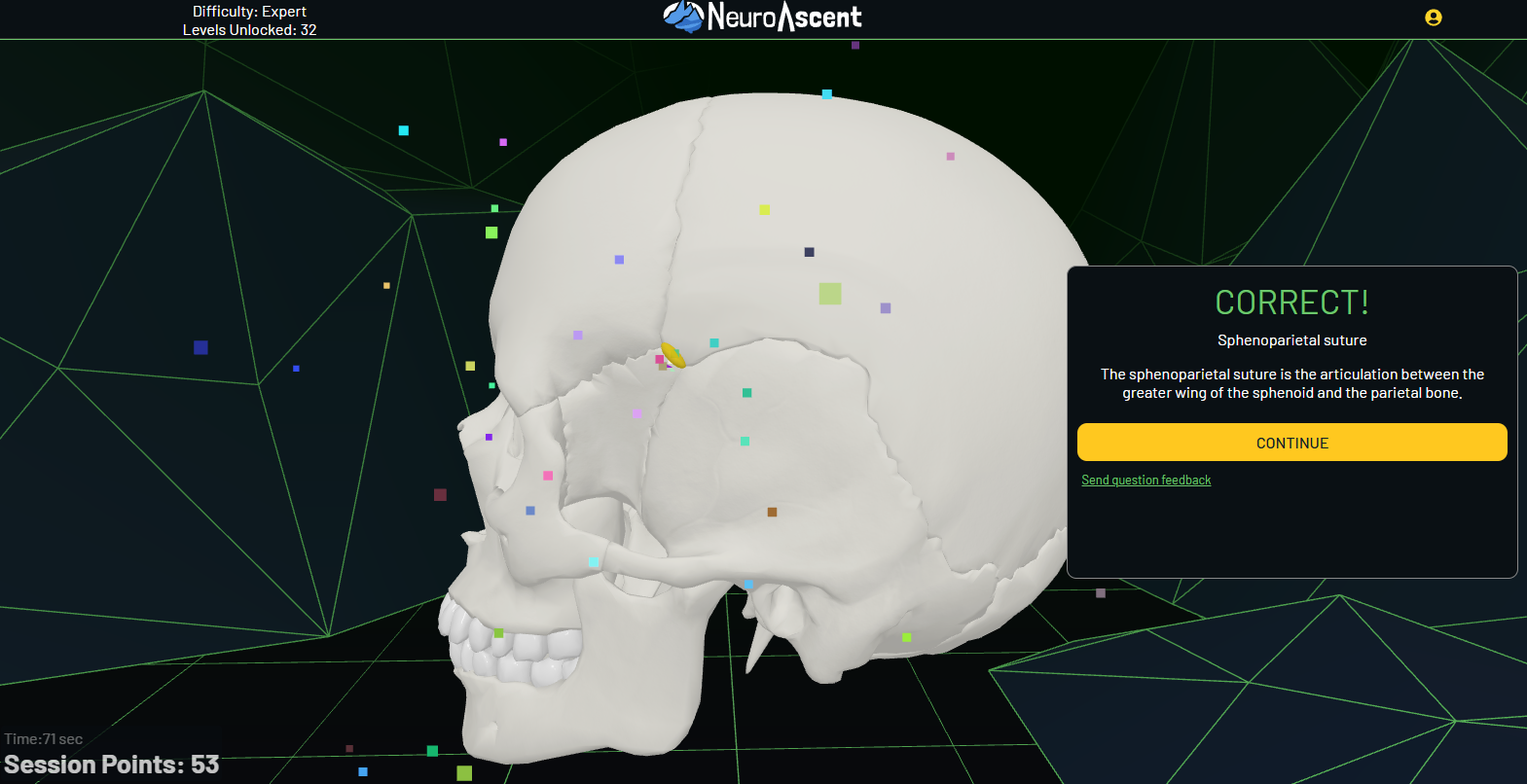
- 3D models let students rotate, zoom, and interact with brain structures in ways that 2D illustrations can’t match. This is a big deal for a subject where spatial relationships are everything.
- Games can introduce concepts gradually, moving from basic identification to clinical correlations as the student progresses.
- Instant feedback helps students catch misunderstandings before they solidify.
- Competitive elements like leaderboards and timed modes add motivation that textbooks don’t provide.
Tools already in use include VR and AR simulations for spatial exploration of brain anatomy, interactive quiz platforms, and collaborative online environments where learners compete or work together. NeuroAscent combines several of these approaches, pairing 3D models with spaced repetition and game mechanics to make neuroanatomy more accessible.
What the Research Shows
The academic evidence for GBL in medical education is growing, though the results aren’t uniformly positive. Chariker et al. (2011) demonstrated in the Journal of Educational Psychology that 3D interactive models improved spatial understanding of neuroanatomy, a skill that’s hard to build from textbooks alone. But Khot et al. (2013) found in Anatomical Sciences Education that computer-based resources weren’t superior to traditional models, which suggests digital tools work best as supplements, not replacements.
On the spaced learning side, Kerfoot (2010) showed in a randomized controlled trial that adaptive spaced education delivered via email improved learning efficiency among medical trainees. And a systematic review by Graafland et al. (2012) in the British Journal of Surgery examined serious games for surgical skills training, finding evidence of their potential to support both engagement and performance.
So the overall picture is encouraging but not simple. GBL isn’t a replacement for traditional teaching, and nobody serious is claiming it should be. But as a supplement, particularly for spatially complex subjects like neuroanatomy, the evidence supports its value.
References
Sailer M, Homner L. The Gamification of Learning: a Meta-analysis. Educ Psychol Rev. 2020;32(1):77-112. doi:10.1007/s10648-019-09498-w.
Garris R, Ahlers R, Driskell JE. Games, Motivation, and Learning: A Research and Practice Model. Simul Gaming. 2002;33(4):441-467. doi:10.1177/1046878102238607.
Chariker JH, Naaz F, Pani JR. Computer-based learning of neuroanatomy: a longitudinal study of learning, transfer, and retention. J Educ Psychol. 2011;103(1):19-31. doi:10.1037/a0021095. PMID: 23349552.
Khot Z, Quinlan K, Norman GR, Wainman B. The relative effectiveness of computer-based and traditional resources for education in anatomy. Anat Sci Educ. 2013;6(4):211-215. doi:10.1002/ase.1355. PMID: 23509000.
Kerfoot BP. Adaptive spaced education improves learning efficiency: a randomized controlled trial. J Urol. 2010;183(2):678-681. doi:10.1016/j.juro.2009.10.005. PMID: 20022032.
Graafland M, Schraagen JM, Schijven MP. Systematic review of serious games for medical education and surgical skills training. Br J Surg. 2012;99(10):1322-1330. doi:10.1002/bjs.8819. PMID: 22961509.